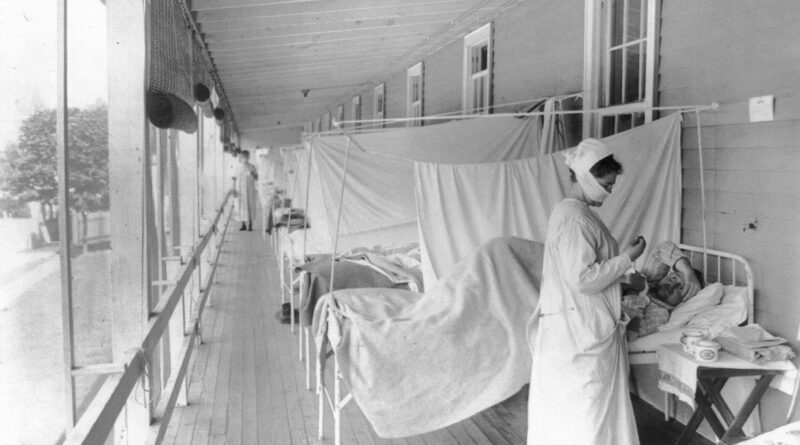
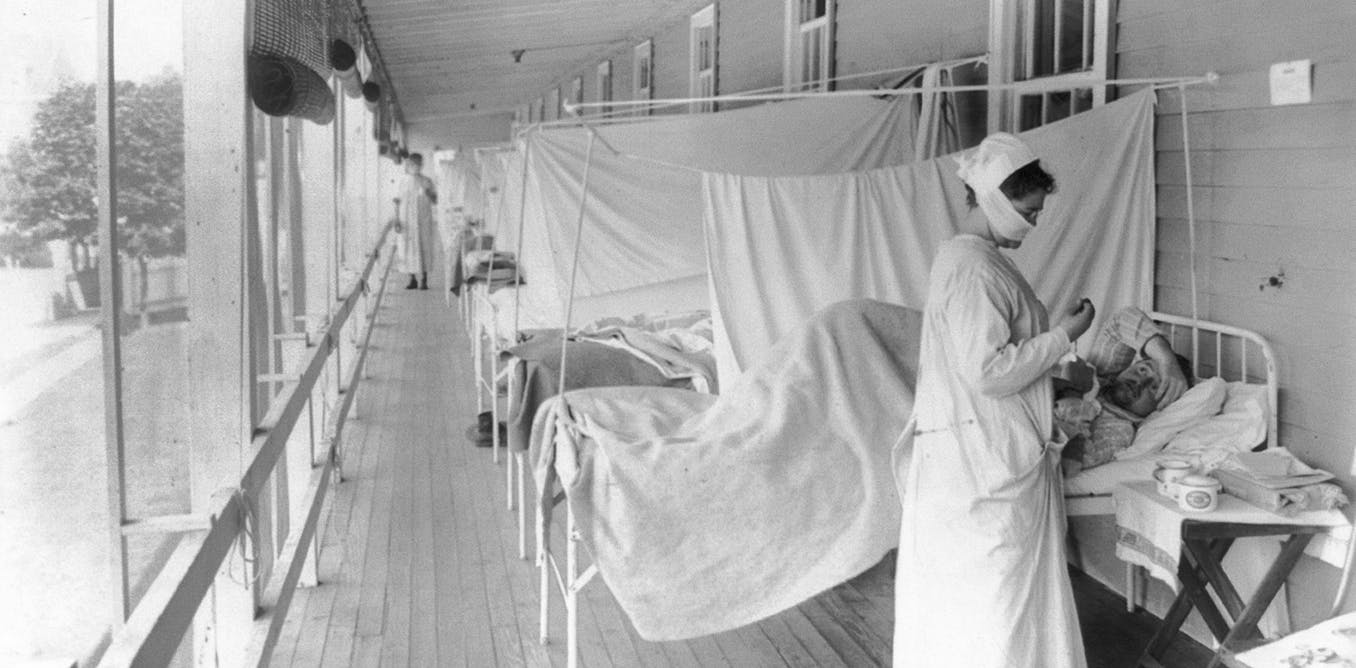
1918 flu pandemic upended long-standing social inequalities – at least for a time, new study finds
The Research Brief is a short take about interesting academic work.
The big idea
Racial disparities in influenza deaths shrunk by 74% in U.S. cities during the 1918 flu pandemic due to an odd coincidence of virus and history. That’s the key finding of our recently published study in the journal Demography.
This conclusion contradicts the common claim that crises like pandemics make social inequalities worse. The 1918 influenza pandemic was a surprising exception.
Prior to the 1918 pandemic, Black people in the U.S. died of respiratory diseases at vastly higher rates than white people. But our study found that urban white people in their 20s and 30s were especially vulnerable to the 1918 virus, dying at rates that were up to 20 times higher than normal. While the death rates of Black people in urban settings also spiked during the 1918 pandemic, they did so by a much smaller rate than in white populations. On average, across all age groups, white mortality increased fivefold, while Black mortality increased threefold.
Overall, Black people still died at higher rates than white people during the 1918 pandemic, but the ratio of Black-to-white mortality – a measure of racial inequality – shrank dramatically compared with other time periods. So while 1918 was wildly deadly across the world, the death rate among urban white young adults in the U.S. was truly unprecedented.
Why it matters
One anomalous feature of the pandemic is well known: It killed many young adults alongside children and elderly people, who are traditionally at risk from flu viruses.
But the unusually small racial inequality in flu deaths in the U.S. in 1918 is a little-known puzzle that contrasts with modern pandemics like COVID-19 and HIV, which have hit Black communities especially hard. It also contrasts with a global tendency for poorer populations to be more likely to die from the flu.
Our study considered several hypotheses to explain the surprising patterns in the U.S. during the 1918 pandemic. One such potential explanation was that policies like school closures especially benefited Black populations because of their higher risk of dying from the flu in nonpandemic years when such measures were absent.
But only one explanation fits our evidence: Urban white young adults in the U.S. were deeply vulnerable in 1918 because of the way their immune systems had been programmed during childhood in the late 19th century. This is because the first flu people encounter as children is special: It teaches the immune system how to respond to future flu infections. However, research shows that this so-called immunological imprinting can be harmful when the virus someone later encounters is very different from the virus their immune system has been trained against.
The last flu pandemic to hit U.S. cities before 1918 was a devastating global pandemic that began in 1889. Exposure to that virus would have taught children’s immune systems to expect what was probably an H3N8 flu. But the devastation in 1918 was caused by the world’s first H1N1 pandemic. The two strains belong to two different groups of influenza viruses, and immune protection from H3N8 would not have conferred protection against H1N1.
To the contrary: People whose first flu exposure occurred in the 1890s would have likely had a compromised immune response to the 1918 pandemic because their immune system produced the wrong kind of antibodies that crowded out more effective ones.
In 2013 and 2014 studies, two groups of virologists and demographers proposed and tested the hypothesis that 1890s imprinting explains the unusually high mortality of young adults during the 1918 pandemic. We adapted their argument to explain unusually small racial disparities as well.
This hypothesis suggests that the pattern of Black and white deaths in 1918 revolves around a historical coincidence. Black young adults were more often spared this fateful imprinting because they spent their childhoods in rural areas. As a result, though they often lived in deep poverty, they did not encounter some of the respiratory diseases that were rampant in cities. So while they were vulnerable to 1918’s novel flu, they were less so than people whose immune systems were primed to meet a virus like the one that circulated in the 1890s.
What still isn’t known
Immunologists are only beginning to understand the exact mechanisms through which imprinting affects long-term immune responses. Recent studies about the early 20th century and the COVID-19 pandemic support the idea that imprinting can significantly affect immune responses later in life. We all carry in our bodies the memories of our past disease exposures.
Those exposures changed radically during the 20th century, and the full consequences for population immunity in the COVID-19 era remain to be unraveled.